Testicular Cancer: Let’s Talk About It
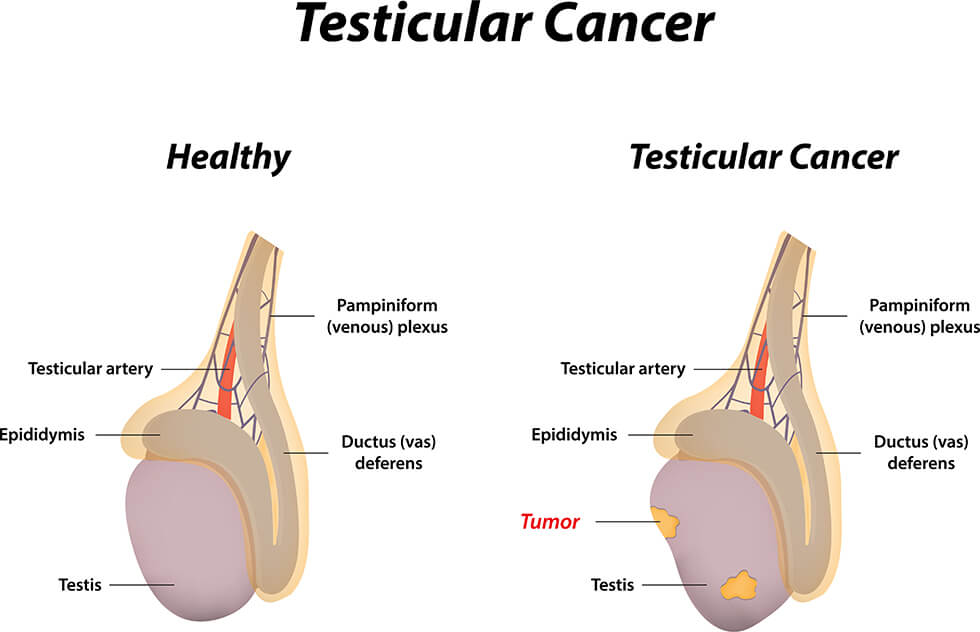
Testicular cancer occurs when abnormal cells in one or both testicles multiply uncontrollably, forming a malignant tumor. The testicles, located in the scrotum, play a vital role in producing sperm and testosterone.
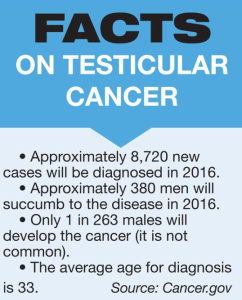
Although testicular cancer is a serious disease, it is relatively rare, affecting approximately 1 in 250 individuals with testicles in their lifetime. Notably, it is the most prevalent form of cancer among individuals assigned male at birth between the ages of 15 and 35.
Despite its rarity, testicular cancer is highly treatable and curable, making early detection and awareness crucial for effective management and treatment.
RISK FACTORS

Four primary risk factors increase the likelihood of developing testicular cancer:
- Cryptorchidism (undescended testicle): A history of cryptorchidism is the most common risk factor. The abnormal testicular descent may indicate an underlying testicular abnormality, making cancer more likely.
- Family history: Having a brother or father with testicular cancer significantly increases the risk (8-12 fold and 2-4 fold, respectively).
- Personal history: Men with a previous testicular cancer diagnosis have the highest risk of developing another cancer (12-fold increase).
- Intratubular germ cell neoplasia (ITGCN): GCNIS, a precursor lesion, is present in 80-90% of testicular cancer patients. Men with GCNIS have a 50% risk of developing testicular cancer within five years and 70% within seven years.
Note: Microlithiasis, or small calcifications in the testicle, is not a standalone risk factor but may indicate a higher risk when combined with other factors. Regular self-examination and medical follow-up are recommended in such cases.
SYMPTOMS
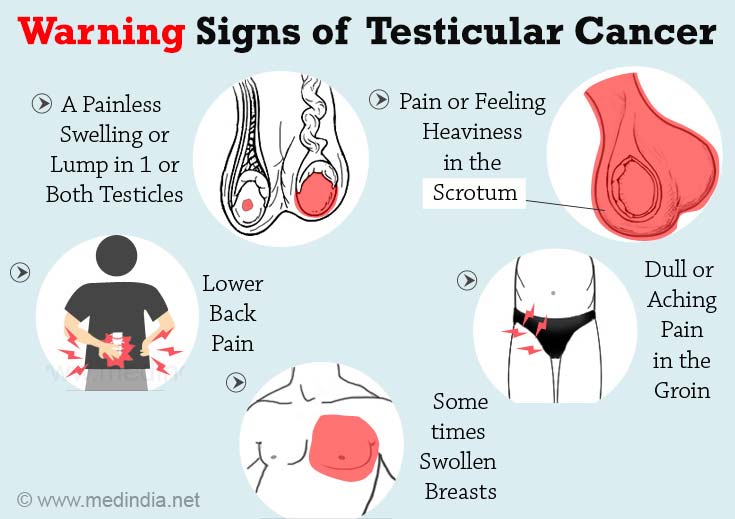
Testicular cancer can be challenging to detect, but being aware of the signs can lead to early diagnosis and treatment. Common symptoms include:
- Painless lumps or swelling in the testicle
- Feeling of heaviness or dull ache in the testicle, scrotum, or groin
- Tenderness or changes in breast tissue
If you notice any unusual lumps or firmness in your testicle, consult a doctor promptly. About 75% of men with testicular lumps or swelling are diagnosed with cancer. However, most masses outside the testicle are non-cancerous.
Don’t hesitate to discuss your symptoms with your doctor or urologist if you experience:
- Lumps lasting longer than two weeks
- Unexplained swelling or pain
Your doctor will investigate the cause and rule out other conditions, such as:
- Epididymitis (inflammation of the epididymis)
- Testicular torsion (twisting of the testicles)
- Inguinal hernia (intestinal protrusion through weakened stomach muscles)
- Hydrocele (fluid buildup in the scrotum)
Early detection and consultation with a medical professional can significantly improve treatment outcomes.
TYPES

Testicular cancer arises from various cell types, each with distinct treatment approaches and prognoses. Accurate diagnosis requires identifying the cell of origin and cancer type.
Germ Cell Tumors (GCTs): The Most Common Type
- Over 90% of testicular cancers originate from germ cells, responsible for sperm production
- Main types: seminomas and non-seminomas, occurring equally
- Mixed germ cell tumors contain both seminoma and non-seminoma cells, treated as non-seminomas
Seminomas: Slow-Growing and Less Aggressive
- Classical (typical) seminomas: most common, typically affecting men aged 25-45
- Spermatocytic seminomas: rare, slower-growing, and less likely to spread, often occurring in older men (average age 65)
Non-Seminomas: Faster-Growing and More Aggressive
- Typically affect men in their late teens to early 30s
- Four main subtypes:
– Embryonal carcinoma
– Yolk sac carcinoma
– Choriocarcinoma
– Teratoma
– Often mixed with other types, including seminoma cells, but treatment remains similar for most non-seminoma cancers
Tumor markers like human chorionic gonadotropin (HCG) aid in diagnosis and monitoring treatment response.
Non-seminomas are aggressive testicular cancers with distinct subtypes:
- Embryonal Carcinoma (40% of testicular tumors):
- – Rarely occurs as a pure form (3-4%)
- – Microscopically resembles early embryo tissues
- – Rapid growth and spread outside the testicle
- – Increases alpha-fetoprotein (AFP) and human chorionic gonadotropin (HCG) levels
- Yolk Sac Carcinoma:
- – Most common in children, especially infants
- – Rare in adults, with a poorer prognosis
- – Responds well to chemotherapy, even with spread
- – Almost always increases AFP levels
- Choriocarcinoma:
- Extremely rare and fast-growing in adults
- Pure form likely to spread rapidly to other body parts
- Often found with other non-seminoma cells in mixed tumors
- Increases HCG levels
- Teratoma:
- – Rare as a pure form
- – Composed of cells resembling embryonic layers
- – Three main types:
– Mature Teratoma: rare spread, curable with surgery, but may recur
– Immature Teratoma: more aggressive, invasive, and metastatic
– Teratoma with Somatic Type Malignancy: very rare, with mixed cell types
Testicular germ cell cancers can begin as a non-invasive condition called carcinoma in situ (CIS) or intratubular germ cell neoplasia. In CIS, abnormal cells are confined within the seminiferous tubules, where sperm cells are produced. CIS may not always progress to invasive cancer, but it’s challenging to detect due to the absence of symptoms or palpable lumps. Biopsy is the only definitive diagnostic method.
Treatment approaches for CIS vary among experts, with some recommending observation (watchful waiting) due to the uncertain progression to invasive cancer.
Invasive cancer develops when CIS cells breach the seminiferous tubules and infiltrate other testicular structures, potentially spreading to lymph nodes or distant organs via lymphatic vessels or blood.
Stromal Tumors: A Rare Type
Gonadal stromal tumors originate in the supportive and hormone-producing tissues of the testicles, accounting for less than 5% of adult testicular tumors and up to 20% of childhood cases. The primary types are:
- Leydig Cell Tumors:
- Arise from cells producing male sex hormones (androgens)
- Can occur in adults and children
- Often produce androgens, but sometimes estrogens
- Mostly benign, with rare cases spreading to other body parts and resisting chemotherapy and radiation therapy
- Sertoli Cell Tumors:
- Originate from normal Sertoli cells, which support and nourish sperm-making germ cells
- Typically benign, but can be aggressive if they spread
- Poor response to chemotherapy and radiation therapy if they metastasize
Secondary Testicular Cancers:
- Cancers that originate in another organ and spread to the testicle
- Not considered true testicular cancers, as they don’t start in the testicles
- Named and treated based on their primary origin
- Examples:
– Lymphoma (most common secondary testicular cancer)
– Leukemia (can form a testicular tumor in boys)
– Prostate, lung, skin (melanoma), kidney, and other organ cancers (poor prognosis due to widespread metastasis).
DIAGNOSIS
Testicular cancer can be identified through self-examination, a healthcare provider’s exam, or a combination of both. To confirm the diagnosis, several tests are necessary:
- Ultrasound Imaging:
– Uses sound waves to create images of the scrotum and testicles
– Helps differentiate between cancerous and non-cancerous lumps
– Determines the location of lumps (inside or outside the testicle)
– Lumps inside the testicle are more likely to be cancerous
- Blood Tests (Tumor Marker Tests):
– Detect proteins produced by testicular cancer cells
– Measure levels of beta-human chorionic gonadotropin, alpha-fetoprotein, and lactate dehydrogenase
– Elevated levels can indicate testicular cancer, but are not definitive proof
- Surgical Removal of the Testicle (Orchiectomy):
– Performed if a lump is suspected to be cancerous
– The removed testicle is sent to a laboratory for examination
– Confirmatory testing determines the presence of cancer cells
IDENTIFYING TESTICULAR CANCER TYPE
To determine the specific type of testicular cancer, your healthcare team conducts tests on the cancer cells. This information guides treatment decisions. The most common testicular cancer types are:
- Seminoma:
– Typically occurs at an older age
– Slower-growing and spreading compared to nonseminomas
- Nonseminoma:
– Often occurs at a younger age
– Aggressive growth and rapid spread
– Subtypes include:
– Choriocarcinoma
– Embryonal carcinoma
– Teratoma
– Yolk sac tumor
DETERMINING TESTICULAR CANCER STAGE
After diagnosis, your healthcare team assesses the cancer’s extent to determine its stage. Staging helps predict prognosis and guides treatment decisions. Tests used for staging include:
- Computerized Tomography (CT) Scan:
– Takes X-ray images of the abdomen, chest, and pelvis
– Helps identify potential cancer spread
- Blood Tests (Tumor Marker Tests):
– Repeated after testicle removal surgery
– Monitors cancer cell presence and guides additional treatment needs
– Used during and after treatment to track progress
Testicular cancer stages range from 0 to 3:
– Stage 0 and 1: Cancer is localized to the testicle and surrounding area, without lymph node or distant spread.
– Stage 2: Cancer has spread to lymph nodes.
– Stage 3: Cancer has spread to other body parts or has high tumor marker levels, indicating potential spread.
Accurate staging is crucial for developing an effective treatment plan and understanding the likelihood of cure.
TREATMENT OPTIONS

Testicular cancer is typically treatable, and the chosen treatment approach depends on:
- Cancer size and type
- Extent of spread
- Overall health
Treatment usually begins with surgical removal of the affected testicle, which may be the only necessary treatment or followed by additional therapies like:
- Chemotherapy
- Radiotherapy
It’s essential to discuss fertility concerns with your healthcare team before starting treatment, as some options may impact fertility. Sperm banking (collecting and storing sperm) will be offered to preserve fertility options.
Your specialist care team will:
- Explain treatment benefits, risks, and side effects
- Collaborate with you to create a personalized treatment plan
- Address fertility concerns and treatment implications
Regular check-ups, tests, and scans will monitor progress during and after treatment. If concerns or side effects arise, don’t hesitate to reach out to your healthcare team – you don’t need to wait for your next scheduled appointment.
Surgery:
- Primary treatment for testicular cancer
- Involves removing the affected testicle (orchidectomy)
- May be the only necessary treatment
- Option to have an artificial testicle implanted
- Rarely, partial orchidectomy (removing part of the testicle) may be performed
- Additional surgery may be required to remove lymph nodes in the abdomen if cancer has spread
- Lung surgery may be necessary if cancer has spread to the lungs
Chemotherapy:
- Uses medication to kill cancer cells
- Administered:
– After surgery to prevent cancer recurrence
– If cancer has recurred or spread to other body parts
Radiotherapy:
- Employs high-energy radiation to kill cancer cells
- Used for specific types of testicular cancer that have spread to abdominal lymph nodes
These treatment options may be used alone or in combination to effectively manage testicular cancer.
Also Read: Chemotherapy: A Whole-Body Approach & Radiation: A Targeted Treatment
Immunotherapy:
Your body’s immune system is a powerful defense against disease, capable of recognizing and attacking harmful cells. However, cancer cells have a clever way of evading this natural protection. Immunotherapy is a ground-breaking treatment that helps your immune system overcome this hurdle, identifying and destroying cancer cells.
In the fight against advanced testicular cancer, immunotherapy emerges as a promising solution when other treatments fall short. By harnessing the strength of your immune system, this innovative approach offers new hope for conquering cancer.
Also Read: What’s new in cancer immunotherapy?
EXCEPTIONAL TESTICULAR CANCER SURVIVAL RATES
Testicular cancer boasts an outstanding survival rate, with:
- Localized cancer (confined to the testicle): 99% five-year survival rate
- Regionalized cancer (spread to nearby lymph nodes and tissues): 96% five-year survival rate
These statistics represent general trends and don’t account for individual factors influencing survival, such as:
- Tumor marker levels
- Cancer type (seminomas tend to be slower-growing and more treatable than nonseminomas)

CONCLUSION
Testicular cancer is a highly treatable and curable form of cancer, with an exceptional survival rate of 99% for localized cancer and 96% for regionalized cancer. Early detection and diagnosis are crucial for effective treatment and improved outcomes. By understanding the risks, symptoms, and treatment options, men can take proactive steps to protect their health and seek medical attention if they notice any unusual changes or abnormalities. With advances in medical research and personalized care, testicular cancer patients can look forward to improved treatment outcomes and enhanced quality of life.