What Is the Gleason Score in Prostate Cancer? Meaning, Stages & Treatment Explained?
Prostate cancer is the second most common cancer in men globally, with over 1.4 million new cases diagnosed worldwide every year. In the United States, one in eight men will be diagnosed with prostate cancer during their lifetime, making it second only to skin cancer in prevalence among American men.
While this may sound alarming, the prognosis is highly favorable when caught early. According to the U.S. Centers for Disease Control and Prevention (CDC), the 10-year survival rate for localized prostate cancer is nearly 100%. This is largely due to increased awareness, effective screening methods, and advances in treatment.
The Gleason score is one of the most important tools for determining how aggressive prostate cancer is. Understanding the Gleason score can help patients and families navigate this diagnosis and make better decisions about the best course of treatment.
What Is Prostate Cancer?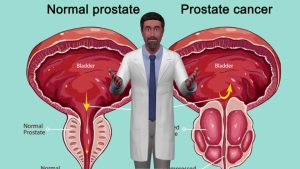
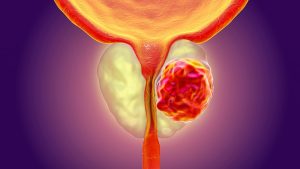
The prostate is a small gland located just beneath the bladder in males. It produces the fluid that goes into making semen and envelops the urethra. Prostate enlargement and, occasionally, the growth of cancerous cells are among the changes that men may experience as they age.
When abnormal cells in the prostate gland start to grow out of control, prostate cancer develops. It often develops slowly and may not cause symptoms in its early stages. However, when symptoms do appear, they may include:
- Recurring or painful urination
- Weak urine stream
- Blood in the semen or urine
- Erectile dysfunction
- Lower back pain or hip pain
Prostate cancer can metastasize, or spread, to bones and other organs if treatment is not received, which drastically reduces survival rates.
What Is the Gleason Score?
The Gleason score is a grading system used to evaluate the appearance of abnormal cancer cells under a microscope. Dr. Donald Gleason created this system in the 1960s, and it is still one of the most crucial ways to determine how aggressive a prostate tumor may be.
How the Gleason Score Works?
Following a prostate biopsy, a pathologist evaluates the two most common patterns of cancer cells and assigns them a score ranging from 1 (least aggressive) to 5. These two numbers are then added to form a Gleason sum, which varies between 6 and 10:
- Gleason 6 or lower: Gleason 6 is the lowest score assigned after biopsy, indicating low-grade cancer with cells similar to normal tissue and low spread potential. Scores below 6 are uncommon, as they indicate near-normal tissue.
- Gleason 7: Intermediate cancer with moderate spreading risk.
- Gleason 8–10: High-grade cancer; cells look highly abnormal and are more likely to spread quickly and metastasize.
Understanding Grade Groups
To simplify the interpretation of the Gleason score, modern guidelines categorize results into Grade Groups:
| Gleason Score | Grade Group | Aggressiveness |
| 6 or below | 1 | Low |
| 3+4=7 | 2 | Favorable intermediate |
| 4+3=7 | 3 | Unfavorable intermediate |
| 8 | 4 | High |
| 9–10 | 5 | Very high |
Note: Depending on which pattern predominates, two patients’ cancers may behave differently even if they have the same Gleason sum (for example, 7). For example, 3+4 is less aggressive than 4+3, though both equal 7.
Gleason Score vs. PSA Test: What’s the Difference?
Two of the most common screening and diagnostic tools in prostate cancer are the Gleason score and the PSA test. While they both provide valuable insights, they serve different purposes:
| Feature | Gleason Score | PSA Test |
| Purpose | Measures cancer cell aggressiveness | Detects prostate-specific antigen levels in blood |
| When Used | After a cancer diagnosis | As a screening tool |
| How It’s Done | Biopsy and tissue examination | Simple blood test |
The amount of prostate-specific antigen (PSA) in the blood is determined by a PSA test. Prostate cancer may be indicated by elevated PSA levels, but benign conditions like prostatitis or an enlarged prostate can also be the cause.
Guidelines for Screening for Prostate Cancer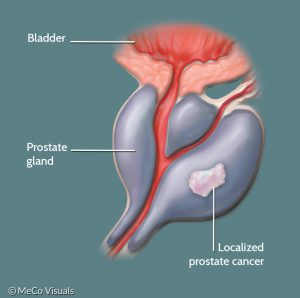
The U.S. Preventive Services Task Force (USPSTF) recommends that each person make their own decision about getting screened for prostate cancer. According to their guidelines:
- Ages 55–69: Discuss the advantages and disadvantages of screening with your physician.
- Ages 70 and above: It is not advised to undergo routine PSA testing.
High-Risk Groups
The American Cancer Society (ACS) recommends earlier screening for high-risk men:
- Age 50: Average risk
- Age 45: High risk (Black men, or those with a first-degree relative diagnosed before age 65)
- Age 40: Extremely high risk (detected early in multiple first-degree relatives)
What is the Significance of the Gleason Score for Treatment?
Dr. Bradford Tan, Chair of Pathology at the Cancer Treatment Centers of America, notes that the Gleason score, along with other diagnostic factors, guides treatment options. Here’s how:
- Gleason 6 (Low risk): May qualify for active surveillance—regular monitoring without immediate treatment.
- Gleason 7 (Intermediate risk): Requires individualized decision-making; options may include surgery, radiation, or hormone therapy.
- Gleason 8–10 (High risk): Often treated aggressively with a combination of hormone therapy, surgery, and radiation.
In some advanced cases, orchiectomy (surgical removal of testicles) or ongoing hormone therapy may be necessary to manage metastatic cancer
Key Prostate Cancer Statistics (Global & India—Latest Data & 2025 Estimates)
| Metric | Global (Latest & Estimated) | India (Latest & Estimated) |
| New Cases Annually | ~1.41 million new cases (GLOBOCAN 2020) 2025 Estimate: ~1.6 million cases | ~34,500 new cases (GLOBOCAN 2020) 2025 Estimate: ~45,000 cases |
| Rank Among Men’s Cancers | 2nd most common globally | 10th most common in India |
| Annual Deaths | ~375,000 deaths/year (2020) 2025 Estimate: ~415,000 deaths | ~16,800 deaths/year (2020) 2025 Estimate: ~22,000 deaths |
| 5-Year Survival Rate (Localized) | >95% in developed nations | ~60–70% (due to late diagnosis) |
| Average Age at Diagnosis | ~66–68 years | ~65–70 years |
| Lifetime Risk (Men) | 1 in 8 (U.S.) and 1 in 15–20 (global average) | Exact data varies; estimates are lower due to underreporting |
| Mortality-to-Incidence Ratio | ~0.26 (Developed countries: lower) | ~0.49 (India; higher due to late-stage detection) |
| Screening & Awareness | High in North America & Europe, Widespread PSA use | Limited awareness, low PSA screening uptake |
| High-Risk Groups | Older men, African ancestry, family history | Urban males, family history, aging population |
| Top Challenges | Overdiagnosis and overtreatment in high-income communities | Limited screening, late-stage diagnosis, and problems with access |
The Importance of Early Detection:
When detected early, prostate cancer is very treatable. For metastatic cases, the five-year survival rate falls to roughly 30%, underscoring the significance of timely screening and routine checkups, particularly for men over 50 or those in high-risk groups.
Conclusion
Understanding your Gleason score is essential in the journey of managing prostate cancer. In addition to resources such as the PSA test and professional advice. The Gleason score is a useful tool for assessing the type and severity of cancer, enabling doctors to customize treatment regimens to patients’ particular conditions. Learning about the Gleason grading system can help you understand whether you are thinking about screening or have just received a diagnosis, and build confidence in making informed health decisions.
FAQs
What is a Gleason score, and why is it important in prostate cancer?
By analyzing the patterns of cancer cells in a biopsy, the Gleason score assesses the aggressiveness of prostate cancer. It helps doctors decide on the best treatment plan and predict how likely the cancer is to spread.
Is a Gleason score of 6 considered cancer?
Indeed, the lowest grade commonly used to diagnose prostate cancer is a Gleason score of 6. It denotes slow-growing, low-grade cancer, which is frequently appropriate for active surveillance instead of immediate treatment.
How does the Gleason score affect prostate cancer treatment?
Depending on the stage and spread of cancer, lower Gleason scores (such as 6) might only require monitoring, whereas higher scores (7–10) frequently call for active treatment like hormone therapy, radiation, or surgery.
What is the difference between a PSA test and a Gleason score?
The Gleason score is used to grade the severity of cancer following a biopsy, whereas the PSA test is a blood test used to screen for prostate cancer. PSA detects potential issues; Gleason guides treatment.
How common is prostate cancer in India and globally?
Prostate cancer is the second most common cancer in men worldwide, with over 1.4 million new cases annually. In India, it’s the 10th most common male cancer, with rising cases due to increased awareness and aging.
- How HPV Leads to Throat Cancer: Risks & Key Facts
- CAR T-Cell Therapy in India: Cost, Availability & What Patients Must Know