

Ewing’s Sarcoma: The Silent Threat to Young Lives
Ewing’s sarcoma is a rare form of cancer that predominantly affects teenagers but can also occur in younger children and young adults. Known also as Ewing’s sarcoma or Ewing tumor, this cancer typically originates in the bones but can also develop in nearby soft tissues. Advances in research and treatment have improved survival rates, allowing more people with Ewing sarcoma to live longer and cancer-free.
TYPES OF EWING SARCOMA
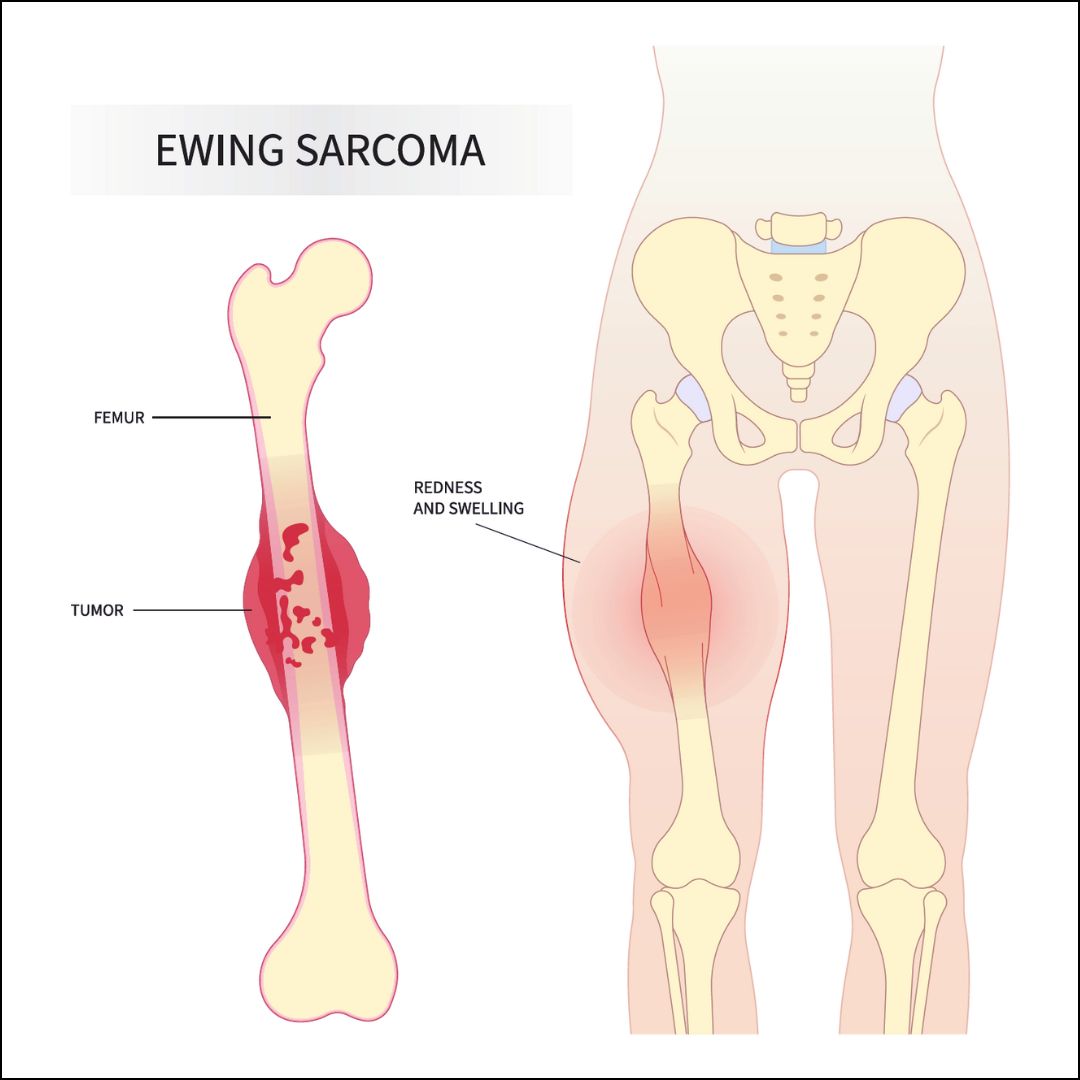
- Ewing’s Sarcoma of Bone: This is the most common type and originates in the bones.
- Extraosseous Ewing Tumor (EOE): This type occurs in the soft tissues surrounding the bones, such as muscles, tendons, and ligaments.
- Peripheral Primitive Neuroectodermal Tumor (PNET): Similar to Ewing sarcoma and EOE in its origins, PNET has a slightly different genetic profile. It can develop in either bone or soft tissue.
CAUSES OF EWING’S SARCOMA
The exact cause of Ewing’s sarcoma is unknown. It does not appear to be hereditary, and there is no known link to diet, lifestyle, or environmental factors. Research suggests that changes in a cell’s DNA that occur after birth may play a role in the development of Ewing’s sarcoma, though the reasons for these genetic changes are not yet fully understood.
SYMPTOMS OF EWING’S SARCOMA
Ewing’s sarcoma can present with several symptoms, which may be mistakenly attributed to other causes, such as sports injuries. Symptoms may include:
- Pain, swelling, or stiffness in the area where the tumor is located.
- A lump near the skin that may feel warm and soft to the touch.
- Persistent low-grade fever.
- Limping or leg pain.
- Bone pain that worsens with exercise or at night.
- Unexplained fractures.
- Unintended weight loss.
- Unusual fatigue.
GENETIC RISK FACTORS FOR EWING SARCOMA
Certain genetic conditions may increase the risk of developing Ewing sarcoma and other sarcomas. Although having one or more risk factors does not guarantee that a child will develop Ewing sarcoma, it can elevate the likelihood. For instance, children with Fanconi anemia might have an increased risk. If you suspect your child may be at risk, consult their doctor for personalized advice and evaluation.
DIAGNOSTIC AND STAGING PROCEDURES FOR EWING SARCOMA
To diagnose and determine the extent (stage) of Ewing sarcoma, a variety of imaging tests and procedures are used to visualize the bones, soft tissues, and surrounding areas. These tests help determine if the cancer has spread and guide treatment planning. Common diagnostic and staging procedures include:
- MRI (Magnetic Resonance Imaging): Utilizes magnets, radio waves, and a computer to create detailed images of the affected area. Also known as nuclear magnetic resonance imaging (NMRI).
- CT Scan (Computed Tomography): Provides detailed cross-sectional images of the body, such as the tumor area or chest. This test may use a contrast dye for clearer images.
- PET-CT Scan: Combines PET and CT scans to provide a comprehensive view of the tumor and any spread. This method offers more detailed information than either scan alone.
- Bone Scan: Detects rapidly dividing cells, such as cancer cells, in the bones using a small amount of radioactive material injected into a vein.
- Bone Marrow Aspiration and Biopsy: Involves removing bone marrow and a small piece of bone to check for cancer spread. This is done by inserting a needle into the hipbone and examining samples under a microscope.
- X-ray: Uses energy beams to produce images of the inside of the body, including the area where the tumor is located.
- Complete Blood Count (CBC): Measures levels of red blood cells, white blood cells, and platelets in the blood, as well as hemoglobin levels and the proportion of red blood cells.
- Blood Chemistry Studies: Analyzes blood samples to measure substances like lactate dehydrogenase (LDH) that may indicate disease. Unusual levels can be a sign of underlying conditions.
BIOPSY FOR DIAGNOSING EWING SARCOMA
To diagnose Ewing sarcoma, a biopsy is performed to obtain tissue samples for microscopic examination by a pathologist. This helps in confirming the presence of cancer. Ideally, the biopsy should be conducted at the same medical center where the treatment will be provided. There are two primary types of biopsies used for diagnosing Ewing sarcoma:
- Incisional Biopsy: Involves removing a sample of tissue through an incision in the skin.
- Needle Biopsy: Uses a needle to extract a tissue sample.
The choice of biopsy method and site is crucial, as an improperly chosen site could lead to complications, requiring more extensive surgery or larger radiation treatment areas.
If there is a concern that the cancer may have spread to nearby lymph nodes, one or more lymph nodes may be removed and examined.
TESTS PERFORMED ON BIOPSY TISSUE
Several tests may be conducted on the biopsy tissue to aid in diagnosis and treatment planning:
- Cytogenetic Analysis: Examines the chromosomes in the tissue sample for abnormalities such as missing, broken, or extra chromosomes, which can indicate cancer. This test helps in diagnosing cancer and assessing the effectiveness of treatment.
- Immunohistochemistry: Uses antibodies to detect specific antigens (markers) in the tissue sample. These antibodies are often linked to enzymes or fluorescent dyes, which become visible under a microscope once they bind to the antigens. This test helps differentiate between different types of cancer.
- Flow Cytometry: Measures the number and characteristics of cells in a sample, including their size, shape, and surface markers. Cells are stained with fluorescent dyes and analyzed as they pass through a light beam. This test provides information on cell properties and tumor markers.
- Molecular Testing: Checks for specific genes, proteins, or other molecules in the tissue, blood, or other fluids. These tests identify gene or chromosome changes associated with Ewing sarcoma.
- Reverse Transcription–Polymerase Chain Reaction (RT–PCR): Measures the amount of messenger RNA (mRNA) produced by specific genes. Using enzymes, this test converts RNA into DNA, amplifies it, and detects gene activation related to cancer presence.
These diagnostic tests are critical for accurate diagnosis and effective treatment planning.
FACTORS AFFECTING PROGNOSIS OF EWING SARCOMA
Before Treatment: Several factors influence the prognosis before any treatment is administered:
- Tumor Location: The specific area in the body where the tumor originated.
- Tumor Type: Whether the tumor is in bone or soft tissue.
- Tumor Spread: Whether the cancer has metastasized to lymph nodes or other distant parts of the body.
- Tumor Size: The size of the tumor at the time of diagnosis.
- LDH Levels: Elevated levels of lactate dehydrogenase (LDH) in the blood.
- Genetic Changes: Presence of specific gene mutations in the tumor.
- Tumor DNA: Detection of tumor DNA in the blood.
- Age and Sex: The patient’s age and sex.
- Previous Cancer Treatment: Whether the patient has undergone treatment for another cancer.
- Initial vs. Recurrent Diagnosis: Whether the tumor is newly diagnosed or has recurred.
After Treatment: The prognosis following treatment is influenced by:
- Surgical Outcome: Whether the tumor was completely removed during surgery.
- Response to Therapy: How well the tumor responded to chemotherapy or radiation therapy.
If Cancer Recurs: Prognosis for recurring cancer depends on:
- Recurrence Timing: Whether the cancer returns more than two years after the initial treatment.
- Recurrence Location: Whether the recurrence is at the original site, in multiple areas, or just one site.
TREATMENT OPTIONS FOR EWING SARCOMA
- Chemotherapy Chemotherapy employs drugs to target and destroy cancer cells by either killing them directly or inhibiting their growth. Administered orally or through injection into the bloodstream or muscles, chemotherapy can reach cancer cells throughout the body (systemic chemotherapy). Typically, a combination of drugs is used (combination chemotherapy). For Ewing sarcoma, systemic combination chemotherapy is a core component of treatment. This approach is often initiated before other treatments like surgery or radiation to shrink the tumor and address any potential spread of cancer cells. The duration of chemotherapy generally spans 6 to 12 months.
- Radiation Therapy Radiation therapy uses high-energy x-rays or other forms of radiation to kill cancer cells or prevent their growth. External radiation therapy involves directing radiation from a machine outside the body toward the cancerous area. It is utilized when surgery isn’t an option or would impact crucial body functions or aesthetics. Radiation therapy may shrink the tumor to minimize surgical intervention, treat residual cancer after surgery, or address tumors that have metastasized. It can also be used palliatively to alleviate symptoms from bone tumors.
- Surgery Surgery aims to remove visible cancerous tissue, often following chemotherapy or radiation. The goal is to excise the entire tumor, and any removed tissue or bone may be replaced with a graft or artificial implant. Post-surgery, additional chemotherapy or radiation (adjuvant therapy) might be administered to target any remaining cancer cells and reduce the risk of recurrence.
- High-Dose Chemotherapy with Stem Cell Rescue This treatment involves administering high doses of chemotherapy to eradicate cancer cells, which also destroys healthy blood-forming cells. To restore these cells, stem cell transplantation is employed. Stem cells, collected from the patient or a donor, are frozen and later reintroduced after chemotherapy. These stem cells regenerate the body’s blood cells. This approach is used for both localized and recurrent Ewing sarcoma.
EMERGING TREATMENTS FOR EWING SARCOMA
- Immunotherapy harnesses the body’s immune system to fight cancer. Here are some approaches currently under investigation:
- CAR T-cell Therapy: This method involves modifying the patient’s T cells, a type of immune cell, to better recognize and attack cancer cells. The T cells are extracted from the patient’s blood and genetically engineered in a lab to express a chimeric antigen receptor (CAR) on their surface. These modified cells are then grown in the lab and infused back into the patient. CAR T-cells are designed to target specific proteins found on cancer cells. Research is ongoing to evaluate the effectiveness of CAR T-cell therapy for treating recurrent Ewing sarcoma.
- Clinical Trials Clinical trials explore new treatments and methods for cancer care. Participation in a clinical trial might be beneficial as these trials test innovative treatments and provide access to cutting-edge therapies. They are crucial for advancing cancer treatment and improving patient outcomes.
- Types of Trials: Clinical trials may involve patients who have not yet started treatment, those whose cancer has not responded to current treatments, or individuals seeking new ways to prevent cancer recurrence or minimize side effects.
- Trial Locations: Clinical trials are conducted across various locations. Detailed information about trials can be found on the NCI’s clinical trials search webpage or the ClinicalTrials.gov website.
MANAGING SIDE EFFECTS AND LATE EFFECTS
Cancer treatment can lead to side effects, both during and after treatment:
- Side Effects During Treatment: These can include various physical and emotional issues. Monitoring and managing these effects are essential for patient well-being.
- Late Effects: Long-term or late effects may manifest months or years after treatment and can include physical problems, emotional or cognitive changes, and an increased risk of secondary cancers. For instance, patients treated for Ewing sarcoma may have a heightened risk of developing acute myeloid leukemia, myelodysplastic syndrome, or new sarcomas in the radiation-treated area.
Bottom of Form
FOLLOW-UP CARE AND TESTING
As your child undergoes treatment for Ewing sarcoma, regular follow-up tests and check-ups are essential. These tests help evaluate the effectiveness of the treatment and guide decisions about whether to continue, adjust, or halt therapy. Some diagnostic tests may be repeated to monitor progress and detect any recurrence of cancer.
Ongoing Monitoring: After treatment, periodic tests will continue to track your child’s condition and identify if the cancer has returned or if there are changes in their health status.
TREATMENT APPROACHES
Localized Ewing Sarcoma: For newly diagnosed localized Ewing sarcoma, standard treatments typically include:
- Chemotherapy: Often the first line of treatment to shrink the tumor.
- Surgery and/or Radiation Therapy: Used to remove the tumor and target remaining cancer cells.
- High-Dose Chemotherapy with Stem Cell Rescue: Involves high-dose chemotherapy followed by the infusion of the patient’s own stem cells to restore blood cell production.
Metastatic Ewing Sarcoma: For newly diagnosed metastatic Ewing sarcoma, treatment usually involves:
- Chemotherapy: To manage cancer that has spread.
- Surgery: To remove tumors if feasible.
- Radiation Therapy: To target cancer cells in specific areas.
Recurrent Ewing Sarcoma: Treatment options for recurrent Ewing sarcoma, where the cancer returns after initial treatment, may include:
- Combination Chemotherapy: To address the cancer comprehensively.
- Surgery: To remove recurring tumors if possible.
- Radiation Therapy: May be used to relieve symptoms and improve quality of life, particularly for bone tumors or in combination with surgery for tumors that have spread.
- High-Dose Chemotherapy with Stem Cell Rescue: To manage recurrent cancer.
CAR T-cell Therapy: An emerging treatment being studied for recurrent cases.
