Craniopharyngioma in Children
Craniopharyngioma is a rare and benign brain tumor that affects the central nervous system (CNS). Because it is located close to important brain structures like the pituitary gland, optic nerves, and hypothalamus, it can still cause major health problems even though it is not cancerous. Although it can happen at any age, it usually affects kids between the ages of 5 and 14.
What Is the Central Nervous System (CNS)?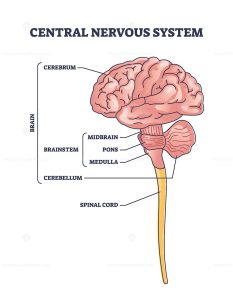
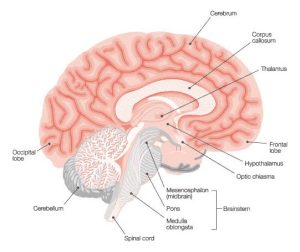
The brain and spinal cord make up the central nervous system (CNS), which regulates thinking, memory, senses, breathing, heart rate, and hormone production. The pituitary gland, located near the tumor site, is the “master gland” responsible for hormone regulation.
What Is Craniopharyngioma?
Craniopharyngiomas are slow-growing brain tumors that are typically found in the suprasellar region, directly above the pituitary gland. It may be cystic, solid, or both. Cystic sections frequently appear clearly on CT or MRI scans and may contain fluid that is rich in proteins.
Despite being benign, the tumor can nevertheless cause serious problems because it puts pressure on surrounding structures, especially in developing children.
Craniopharyngioma Symptoms in Children
Symptoms often appear due to the tumor pressing on nerves, the brain, or hormone-producing glands:
General Symptoms
- Early-morning or chronic headaches
- Nausea or vomiting
- Balance problems
- Excessive fatigue
- Changes in mood or behavior
Symptoms Specific to a Location
- Vision issues or peripheral vision loss
- Excessive thirst and urination (diabetes insipidus)
- Rapid weight gain or obesity
- Early or delayed puberty
- Growth retardation
Note: These symptoms arise due to the tumor’s pressure on the optic nerves, pituitary gland, or hypothalamus, which regulate hormones, metabolism, and visual processing.
Diagnosis: How Is Craniopharyngioma Detected?
Timely diagnosis of Craniopharyngioma is crucial to prevent complications. Your child’s doctor may recommend the following:
Medical History & Physical Exam: The doctor will assess symptoms, growth patterns, and conduct neurological and visual examinations.
Blood & Urine Tests: These help evaluate hormone levels and kidney function. If diabetes insipidus is suspected, a water deprivation test may be conducted.
Imaging Tests: such as MRI Scan (Preferred for visualizing soft tissue detail, size, and tumor spread) or CT Scan to detect calcifications in the tumor and visualize the cystic components.
Biopsy: A biopsy could be carried out if imaging suggests a tumor. A neurosurgeon may perform surgery to remove the entire tumor or just a portion of it. The tissue is then examined by a pathologist to confirm the diagnosis.
Craniopharyngioma Treatment in Children
Treatment is often successful and includes:-
Surgery: Complete or partial removal of the tumor while minimizing damage to surrounding brain structures.
Radiation Therapy: Used if the tumor can’t be fully removed. Risks in radiation therapy include hormone imbalance and memory issues (especially in younger children)
Supportive & Palliative Care: Helps manage symptoms and improve quality of life. It includes hormone therapy, emotional counseling, and physical therapy.
Prognosis and Survival Rate
- The 5-year relative survival rate for children under 15 with craniopharyngioma is 96%.
- Outcomes depend on the child’s age, overall health, and how effectively treatment is administered.
Long-Term Side Effects & Follow-Up Care
Common issues include:
- Hormonal imbalances (requires hormone replacement therapy)
- Gaining weight and becoming obese
- Impairment of vision
- Delays in learning or development
Follow-Up:
- MRI scans for lifelong monitoring
- Neurological and endocrine assessments
- Psychological and nutritional assistance
Rehabilitation:
- Occupational and physical therapy
- Diet Planning
- Emotional and cognitive assistance
- For learning support, school accommodations might also be required.
Emerging Treatments & Research
1. Molecular Subtyping
Craniopharyngiomas have two main subtypes:
- Adamantinomatous (ACP) – Mostly in children; linked to CTNNB1 gene mutations
- Papillary (PCP) – More common in adults; often involves BRAF V600E mutations.
Targeted therapies are being explored based on these molecular profiles.
2. Clinical Trials
Innovations under study include:
- Immunotherapy (e.g., Interferon injections)
- Cyst treatment with bleomycin or radioactive phosphorus
- Better management of obesity and memory decline post-treatment
Talk to your child’s doctor to explore suitable trials and emerging therapies.
Caregiver Support and Resources
A child with a brain tumor requires both physical and emotional care. To manage appointments, prescription drugs, and emotional health, parents and guardians are essential. Make use of the available resources, such as:
- Child life specialists
- Dietitians
- Social workers
- Financial counselors
- Peer support groups
Conclusion
Despite being benign, craniopharyngiomas can have a significant impact. Most children lead healthy lives after treatment if they receive early diagnosis, multidisciplinary care, and lifelong support. Treatment and supportive care advances keep improving results and reducing long-term adverse effects.
FAQs
Is craniopharyngioma cancerous?
No, it is a benign (non-cancerous) tumor, but it can cause serious complications due to its location.
What is the survival rate for childhood craniopharyngioma?
The 5-year relative survival rate is about 96% for children under 15.
What are the early signs of craniopharyngioma in kids?
Common early signs include persistent headaches, vision problems, and unexplained weight gain.
Can a craniopharyngioma return after treatment?
Yes, recurrence is possible. Regular follow-up with MRI scans is essential.
What long-term care is needed after treatment?
Follow-up care may include hormone therapy, weight management, vision monitoring, and psychological support.