CAR T-Cell Therapy India Guide
Cancer treatment in India has come a long way, expanding beyond surgery, chemotherapy, and radiation. Today, targeted therapies and advanced immunotherapy are changing the outlook for many patients. Immunotherapy—often called the fourth pillar of cancer care—helps the body’s own immune system fight cancer, with checkpoint inhibitors, cancer vaccines, and dendritic cell–based treatments leading the progress.
One of the most significant advancements is dendritic cell immunotherapy (Denvax), which helps the immune system recognize and attack cancer cells more accurately. As India adopts newer treatment approaches, options like Denvax dendritic cell therapy are becoming dependable, patient-centered choices for those looking for effective treatment with fewer side effects.
CAR T-cell therapy has shown impressive results in some blood cancers, but its high cost and limited availability make it hard for many patients to access. In contrast, Denvax immunotherapy is more affordable, personalized, and practical for treating solid tumors and cancers that don’t respond well to standard treatments.
Thanks to these innovations, patients in India now have stronger and more focused ways to fight cancer—offering real hope and better outcomes across many cancer types.
What is Car T-Cell Therapy
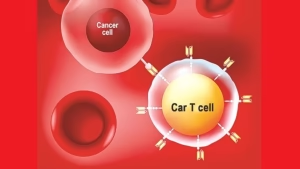
CAR T-Cell therapy is a treatment where a patient’s T cells, a type of immune system cell, are modified in a lab to target and attack cancer cells. T cells are taken from the patient’s blood and engineered with a special receptor called a Chimeric Antigen Receptor (CAR) that binds to a specific protein on cancer cells. These modified CAR T cells are then multiplied in the lab and infused back into the patient’s body. This therapy is used for certain blood cancers and is being researched for other types of cancer as well.

Understanding How CAR T-Cell Therapy Works
The immune system spots threats by looking for antigens—unique markers found on every cell. T cells act as the body’s defenders, using special receptors to identify and attack anything harmful. But sometimes cancer cells slip past them because the T cells don’t have the right receptors to detect them.
CAR T-cell therapy helps fix this by modifying a patient’s own T cells so they can recognize cancer. Doctors collect the T cells, add a gene that forms a chimeric antigen receptor (CAR), and reprogram them to target specific cancer markers like CD19, which is common in leukemia and lymphoma.
After being infused back into the patient, these enhanced CAR T-cells work like precision-targeted fighters, attaching to cancer cells and destroying them. This personalized treatment has become a powerful option for patients with aggressive blood cancers.
Possible Side Effects Of CAR T-Cell Therapy
CAR T-cell therapy is highly potent against certain challenging cancers, yet it may also lead to severe or life-threatening side effects. As a result, it must be administered in specialized medical centers with expertise in its application, and patients require close monitoring for several weeks following CAR T-cell infusion.
Cytokine Release Syndrome (CRS)
- Immune Activation: As CAR T-Cells multiply, they stimulate the immune system, releasing cytokines into the blood.
- Symptoms Recognition: Signs such as fever, chills, breathing difficulties, nausea, vomiting, and fatigue can indicate CRS.
- Early Detection: Doctors are improving their ability to identify CRS promptly, enabling proactive treatment.
Nervous System Concerns
- Neurological Effects: Some patients may experience nervous system complications, manifesting as headaches, confusion, or seizures.
- Vigilance: Monitoring for symptoms like changes in consciousness or tremors ensures timely intervention.
- Patient Safety: Patients are advised against potentially risky activities like driving or operating machinery during the recovery phase.
Other Serious Side Effects
- Infusion Reactions: Allergic responses during treatment are possible but can be managed with appropriate measures.
- Metabolic Imbalances: Monitoring for abnormal mineral levels in the blood, such as potassium or sodium, aids in maintaining balance.
- Immune Suppression: While CAR T-Cell therapy strengthens the immune response against cancer, it may temporarily weaken overall immunity, increasing susceptibility to infections.
- Hematologic Effects: Monitoring blood cell counts helps mitigate risks of infections, fatigue, and bleeding tendencies.
Overall, prompt reporting of any symptoms to healthcare providers is crucial for timely intervention, as various medications are available to address potential side effects, ensuring a smoother treatment journey for patients undergoing CAR T-cell therapy.
What are some of the approved CAR T-cell therapies?
CAR T-cell therapies are authorized by the US Food and Drug Administration (FDA) for the treatment of specific lymphomas, leukemias, and multiple myeloma. Typically, CAR T-cell therapy is considered when other treatment options have been exhausted. Although in certain cases it may even be recommended as the first line of treatment.
Approved CAR T-cell therapies include:
Tisagenlecleucel, also referred to as tisa-cel
Tisagenlecleucel (Kymriah®) is FDA-approved for:
- Treating patients up to 25 years old with B-cell precursor acute lymphoblastic leukemia (ALL) that hasn’t responded to treatment or has relapsed multiple times.
- Treating adults with relapsed or refractory large B-cell lymphoma after trying two or more other treatments, including types like diffuse large B-cell lymphoma (DLBCL).
- Not approved for treating primary central nervous system lymphoma.
- Treating adults with relapsed or refractory follicular lymphoma after trying two or more other treatments. This approval is based on response rate and duration, with ongoing evaluation for full approval.
Axicabtagene ciloleucel, also known as axi-cel
Axicabtagene ciloleucel (YescartaTM) is FDA-approved for:
- Treating adults with large B-cell lymphoma that doesn’t respond to initial chemoimmunotherapy or returns within 12 months after this treatment.
- Treating adults with relapsed or refractory large B-cell lymphoma after trying two or more other systemic therapies, including different types like diffuse large B-cell lymphoma (DLBCL) and primary mediastinal large B-cell lymphoma.
- Not approved for treating primary central nervous system lymphoma.
- Treating adults with relapsed or refractory follicular lymphoma after trying two or more other treatments. Approval is based on initial response rates, with further evaluation needed for full approval.
Brexucabtagene autoleucel, also called brexu-cel
Brexucabtagene autoleucel (Tecartus®) is FDA-approved for:
- Treating adults with mantle cell lymphoma (MCL) that has come back or hasn’t responded to previous treatments. This approval is based on the response rate and how long the response lasts. Further confirmation of clinical benefits may be required in additional studies.
- Treating adults with B-cell precursor acute lymphoblastic leukemia (ALL) that has relapsed or isn’t responding to other treatments.
Lisocabtagene maraleucel, also known as liso-cel
Lisocabtagene maraleucel (Breyanzi®) is FDA-approved for treating adults with large B-cell lymphoma (LBCL), which includes various types like diffuse large B-cell lymphoma (DLBCL), primary mediastinal large B-cell lymphoma, and follicular lymphoma grade 3 B.
Patients who have:
- Disease that doesn’t respond to initial chemoimmunotherapy or relapses within 12 months after this treatment.
- Diseases that doesn’t respond to initial chemoimmunotherapy or relapse after this treatment, and they can’t undergo stem cell transplantation due to other health issues or age.
- Relapsed or refractory disease after trying two or more other treatments.
Breyanzi is not approved for treating primary central nervous system lymphoma.
Idecabtagene vicleucel, also termed ide-cel
Idecabtagene vicleucel (Abecma®) is FDA-approved for adults with multiple myeloma that has returned or isn’t responding to treatment after trying four or more previous lines of therapy. These therapies include an immunomodulatory agent, a proteasome inhibitor, and an anti-CD38 monoclonal antibody.
Numerous other CAR T-cell therapies and similar treatments are undergoing evaluation in clinical trials, with the aim of addressing additional cancer types.
Who Qualifies For CAR T-Cell Therapy?
CAR T-cell therapy represents a revolutionary advancement in cancer treatment, offering hope to individuals facing certain types of leukemia and lymphoma. In the realm of pediatric oncology, CAR T-cell therapy is recommended for children and young people up to the age of 25 diagnosed with a specific form of leukemia known as B-cell acute lymphoblastic leukemia (B-ALL). The therapy is considered in various scenarios:
- Newly Diagnosed Cases: Children and young individuals whose B-ALL persists despite undergoing two cycles of standard treatment protocols may be eligible for CAR T-cell therapy.
- Relapsed Disease Post-Transplant: In cases where B-ALL relapses after a stem cell or bone marrow transplant, CAR T-cell therapy could be considered as an alternative treatment approach.
- Multiple Relapses: Children and young individuals experiencing multiple relapses of B-ALL, even after undergoing prior therapies, may be candidates for CAR T-cell therapy.
- Chemotherapy Resistance: If B-ALL recurs after a period of remission and chemotherapy proves ineffective, CAR T-cell therapy might be explored.
- Ineligibility for Stem Cell Transplant: Individuals whose B-ALL relapses but are deemed unsuitable for a stem cell transplant due to health constraints or lack of a suitable donor may also be considered for CAR T-cell therapy.
On the other hand, CAR T-cell therapy is also available for a subset of adults diagnosed with specific types of lymphoma, including diffuse large B-cell lymphoma, primary mediastinal B-cell lymphoma, and mantle cell lymphoma. Eligibility criteria for adults encompass the following circumstances:
- Disease Persistence or Relapse: Adults with diffuse large B-cell lymphoma or primary mediastinal lymphoma that continues to grow or recurs after at least two rounds of conventional treatments may be considered for CAR T-cell therapy.
- Mantle Cell Lymphoma Resistance: For individuals with mantle cell lymphoma, CAR T-cell therapy might be an option if the disease progresses despite prior treatment with targeted drugs like Bruton’s tyrosine kinase inhibitors (e.g., ibrutinib).
It is imperative to note that CAR T-cell therapy is not a universal solution for all types of cancer. Rather, it is tailored to address specific subtypes of leukemia and lymphoma that exhibit certain molecular characteristics. Moreover, due to its specialized nature and the stringent eligibility criteria, only a limited number of children and adults, approximately 200 adults annually, are deemed suitable candidates for this groundbreaking therapy.
Procedure for CAR T-Cell Therapy
The process of CAR T-Cell Therapy can take weeks:
Collecting the T-Cells
The process begins with the collection of white blood cells, which include the vital T cells, from the patient’s bloodstream. This extraction is performed through a procedure known as leukapheresis. During leukapheresis, patients typically lie comfortably in bed or recline in a chair. To facilitate the process, two intravenous (IV) lines are inserted—one for drawing blood and another for returning it after separation. In certain cases, a specialized IV line called a central venous catheter may be utilized, integrating both IV lines conveniently.
Throughout leukapheresis, patients may need to remain seated or lying down for a duration of 2 to 3 hours. It’s worth noting that there’s a possibility of blood calcium levels dropping during the procedure, which can lead to sensations of numbness, tingling, or muscle spasms. However, healthcare providers can address this by administering calcium supplements orally or through IV infusion.
Making the CAR T-Cells
Following the extraction of white blood cells, the next phase involves isolating the T cells and transporting them to the laboratory for modification. This modification entails the addition of a specific gene encoding the chimeric antigen receptor (CAR), thereby transforming the T cells into CAR T-Cells. Subsequently, these engineered cells undergo a cultivation process, where they’re nurtured and multiplied within the lab environment. It’s important to note that this proliferation process may span several weeks to generate the requisite number of CAR T-Cells essential for therapy.
Receiving the CAR T-Cell infusion
Once a sufficient quantity of CAR T-Cells has been cultivated, they are ready to be reintroduced into the patient’s body through infusion. In preparation for this infusion, patients may receive a course of chemotherapy a few days prior. This pre-infusion chemotherapy serves to suppress the activity of other immune cells, thereby creating a conducive environment for the CAR T cells to exert their anti-cancer effects.
Importantly, the chemotherapy administered is typically mild, as CAR T cells demonstrate optimal efficacy when there are still residual cancer cells to target. Upon infusion, the CAR T-cells commence binding with cancer cells, triggering their activation and subsequent proliferation. This proliferation process enables the CAR T cells to mount a robust attack against the cancer, ultimately aiding in the destruction of malignant cells within the body.
Advancements and Challenges in CAR T-Cell Therapy
CAR T-Cell therapy has shown remarkable potential in clinical trials for patients with blood cancers. In studies, up to 90% of children and adults with B-cell acute lymphoblastic leukemia (B-ALL), who had relapsed multiple times or didn’t respond to standard treatments, achieved remission after receiving CAR T-cell therapy. However, some challenges exist, such as relapses due to tumor cells losing the CD-19 antigen or limitations in CAR T-cell persistence.
Research also indicates promise for CAR T-Cell therapy in other blood cancers like chronic lymphocytic leukemia (CLL) and multiple myeloma. Additionally, investigations are ongoing to explore its effectiveness in treating solid tumors.
Although most patients in CAR T-Cell trials have only been followed for a short time, early response data are emerging rapidly. Long-term follow-up will provide insights into response duration. Enrolling more patients, both pediatric and adult, in clinical trials is crucial for better understanding therapy impact, reducing toxicity, and managing side effects effectively.
10 Questions To Ask Your Healthcare Provider
To be informed about what therapy and treatment you are undergoing is a good thing for your better understanding and problem-solving. Therefore, these are 10 basic questions you should be asking your healthcare provider regarding your CAR T-Cell Therapy:
- What specific type of cancer am I being treated for with CAR T-Cell therapy?
- Can you explain how CAR T-Cell therapy works and how it will benefit my treatment?
- What are the potential risks and side effects associated with CAR T-Cell therapy?
- How will my eligibility for CAR T-Cell therapy be determined?
- What alternative treatment options are available if CAR T-Cell therapy is not suitable for me?
- How many CAR T-Cell therapy procedures have you performed, and what is your experience with this treatment?
- What is the expected timeline for my CAR T-Cell therapy treatment, including preparation, infusion, and recovery?
- How will my response to CAR T-Cell therapy be monitored and evaluated?
- Are there any lifestyle changes or precautions I should take before, during, or after CAR T-Cell therapy?
- What support services are available to my family and me during and after CAR T-Cell therapy, both medically and emotionally?

Final Note
CAR T-cell therapy represents a revolutionary leap in cancer treatment, offering hope and potential remission for patients battling certain types of leukemia and lymphoma. While its efficacy has been demonstrated in clinical trials, challenges such as managing side effects and ensuring long-term response durability persist. However, with ongoing research and advancements, CAR T-Cell therapy continues to evolve, promising improved outcomes and expanded application in the fight against cancer. Engaging with healthcare providers and asking pertinent questions can empower patients to make informed decisions and navigate their CAR T-Cell therapy journey with confidence and clarity.
- Immunotherapy For Cancer In India- A Complete Guide
- Immunotherapy for Prostate Cancer: Types and side effects